坤灵最新logo-scaled-1.png)
Over time, hospital pathology departments often require upgrades. In many cases, these needs result from increased workload, new technologies, or higher safety standards. As a result, additional fume hoods, biological safety cabinets, or large instruments are introduced.
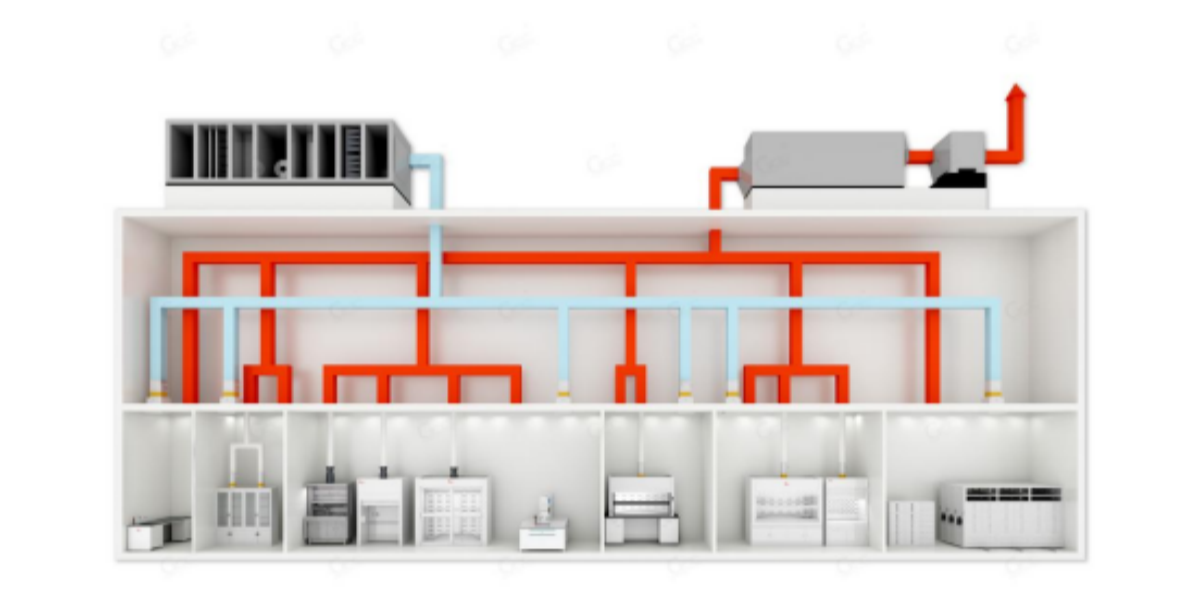
However, most existing ventilation systems are fixed air volume (CAV) systems. They were designed specifically for the original operational load. Therefore, when high-exhaust equipment is added suddenly, the system may exceed its capacity.
As a consequence, several issues can occur. Rooms may lose negative pressure or even become positive. Meanwhile, fume hood face velocity may drop, allowing hazardous gases to escape. In addition, the performance of existing equipment can decline. Noise levels and energy consumption may increase. In extreme cases, pressure monitoring and alarm systems may fail.
For these reasons, simply installing a larger fan is not a safe solution. Instead, a systematic and carefully engineered retrofit is required. In the following sections, the complete process is explained, from diagnosis to commissioning.
Step 1: Comprehensive Diagnosis and Accurate Assessment
Before any modification begins, a detailed system assessment is essential. First, the actual ventilation demand must be clearly understood.
Load Calculation
- Additional Loads: First, calculate the exhaust airflow and heat load of each new fume hood, biological safety cabinet, or device.
- Existing Loads: Next, reconfirm the design or measured exhaust airflow of all current equipment, including grossing stations and tissue processors.
- Room Ventilation Demand: Finally, determine the minimum exhaust airflow required to maintain negative pressure, based on standards such as ≥12 air changes per hour.
System Capacity Evaluation
- Fan Performance: At this stage, review the rated airflow, static pressure, and motor power of supply and exhaust fans. In particular, confirm that they can operate safely under the new conditions.
- Ductwork Capacity: Meanwhile, examine the size and layout of main ducts and branch ducts. Using airflow simulations, resistance increases and bottlenecks can be identified. In most cases, the main duct becomes the limiting factor.
- Control System: In parallel, determine whether the system operates as CAV or VAV. At the same time, verify the condition and accuracy of valves, sensors, and actuators. Expansion capability should also be confirmed.
- Safety Impact: Finally, assess operational risks during construction. Especially during airflow shutdowns, detailed contingency plans must be prepared.
Step 2: Developing a Scientific Retrofit Strategy
Based on the assessment results, different retrofit solutions can be selected. In practice, these options are often combined.
Option A: Optimization and Adjustment
(For minor load increases with available system margin)
In this case, fan speed can be increased within safe limits. At the same time, damper positions are optimized. Airflow is then redistributed to high-risk areas first.
This option is cost-effective and fast. However, capacity improvement is limited. Additionally, noise and energy consumption may increase.
Option B: Core Equipment Upgrade
In many projects, this is the most reliable solution. Existing fans are replaced with higher-capacity, high-efficiency models such as EC fans.
Meanwhile, supply air units are upgraded or added. As a result, make-up air remains balanced and room pressure stays stable.
Overall, this option provides significant and predictable performance improvement.
Option C: Ductwork Modification
When fan capacity is sufficient, ductwork may still limit airflow. In such cases, duct upgrades become necessary.
Initially, branch ducts near new equipment can be upsized. If this is not sufficient, main duct replacement may be required.
However, this approach demands careful planning due to space constraints and downtime risks.
Option D: Intelligent Control System Upgrade
Most importantly, the system can be upgraded from CAV to VAV.
With this approach, VAV boxes and pressure-independent controllers are installed for each hood and room.
During operation, airflow is adjusted in real time based on sash position and room pressure.
When hoods are closed, exhaust airflow is reduced automatically. Consequently, saved airflow capacity is reassigned to new equipment.
Although initial investment is higher, energy savings often exceed 50%. Therefore, long-term returns are substantial.
Option E: Exhaust Air Treatment Expansion
As exhaust airflow increases, treatment demand also rises. Accordingly, activated carbon filters, PCO units, or scrubbers must be reassessed.
If necessary, these systems should be expanded to ensure continued compliance with emission standards.
Step 3: Rigorous Implementation and Commissioning
During construction, a phased approach is critical. First, new systems are installed. Only then are existing systems disconnected.
This method minimizes downtime. In most hospitals, critical switchover work is scheduled at night or on weekends.
Meanwhile, temporary exhaust fans or air cleaners may be deployed. In this way, negative pressure can be maintained in high-risk areas such as grossing rooms.
After installation, full system balancing must be performed. Specifically, hood face velocity, room pressure, and airflow rates are remeasured.
Only after all parameters meet design targets can the system be accepted.
Finally, smoke visualization tests are conducted to confirm airflow direction. At the same time, staff training is provided, especially for VAV operation and alarm response.
Step 4: Key Pre-Retrofit Considerations
Before implementation, regulatory approval is required. Typically, hospital infection control and facilities departments must review the plan. In some cases, environmental authorities are also involved.
From a financial perspective, both capital cost and operating cost must be evaluated. Although VAV systems require higher initial investment, they often deliver strong long-term energy savings.
In addition, future development should be considered. For this reason, designs should reserve 10–20% additional airflow capacity or spare duct connections.
Conclusion
In summary, ventilation expansion in a pathology department is a system-level engineering project. It affects airflow organization, biosafety control, and energy management. Therefore, it should never be treated as a simple fan replacement.
Whenever possible, upgrading from a fixed air volume system to a variable air volume system is recommended. By doing so, the department’s “breathing” becomes flexible and efficient.
As a result, current demands are safely met, and future growth is supported. Ultimately, this ensures long-term biosafety, stability, and compliance.
The final objective is clear:
to keep this invisible safety barrier operating continuously, quietly, and reliably.